
Category Archives: Τηλεσκοπικοί ενδομυελικοί ήλοι
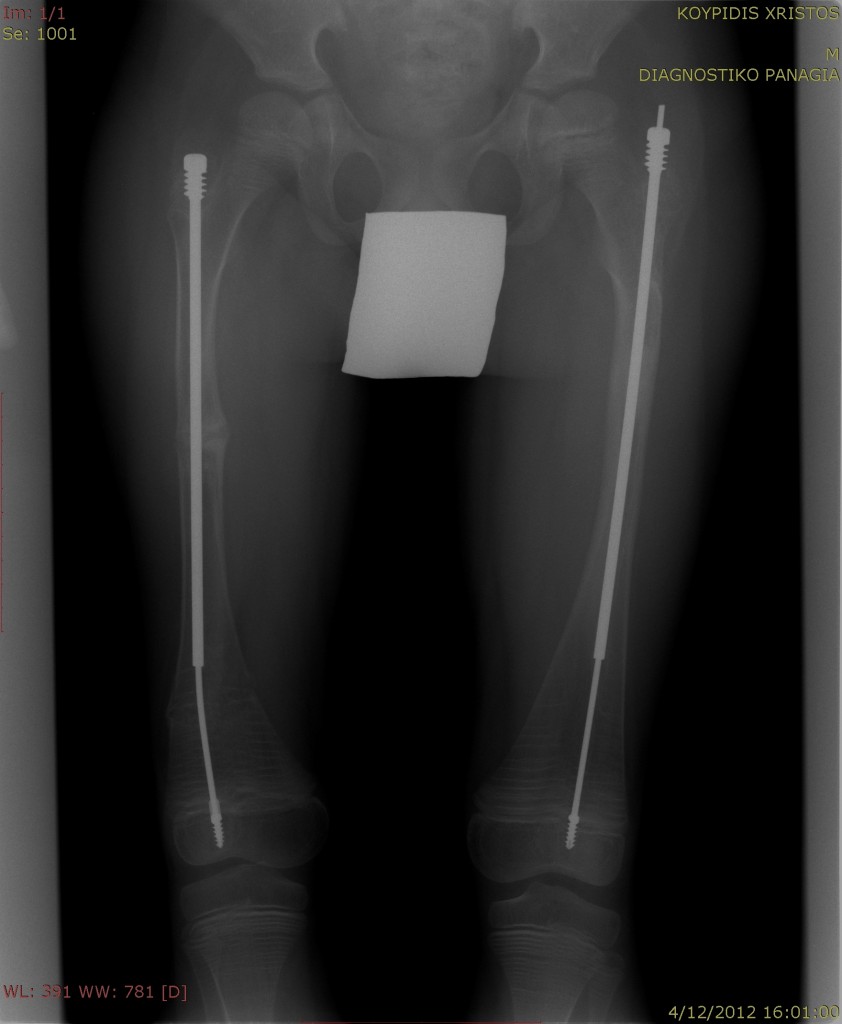
Άσχημα τα νέα..
Χτες βγάλαμε ακτινογραφίες των μηριαίων οστών του Χρήστου μετά το κάταγμα στο δεξί μηρό πριν από 3 εβδομάδες.
Continue reading
Δεν επιτρέπεται σχολιασμός στο Άσχημα τα νέα..
Filed under 2012, Δεκέμβριος, κάταγμα, νέα, Τηλεσκοπικοί ενδομυελικοί ήλοι, Χρήστος
Ακτινογραφίες αριστερού βραχιόνιου
Δεν επιτρέπεται σχολιασμός στο Ακτινογραφίες αριστερού βραχιόνιου
Filed under 2012, ακτινογραφίες, κάταγμα, νέα, Σεπτέμβριος, Τηλεσκοπικοί ενδομυελικοί ήλοι, Χρήστος
Why are F-D rods are better?
Leg rod helps strengthen kids fragile bones
Canadian team's telescopic rod surgery is less invasive, less painful
By Andrew SkellyNEW ORLEANS ? A telescopic rod invented by a pair of Canadian orthopedic surgeons shows promise in strengthening the femurs of children with osteogenesis imperfecta, potentially with fewer complications and reoperations than the traditional technique. The device is attracting attention from as far away as Kuwait, Peru and Sweden. It was developed by Drs. Fran?ois Fassier and Pierre Duval, along with Pega Medical, a Montreal firm specializing in orthopedic devices. In an interview at the meeting here, Dr. Fassier, a pediatric orthopedic surgeon and chief of staff at Shriners Hospital for Children in Montreal, said he even travelled to Slovenia last year to perform the operation on a girl whose family had heard about the operation through word of mouth. ?Everything went very well and I had a Christmas card from the family saying that she's running now,? said Dr. Fassier, who is also an associate professor of surgery at McGill University. The Shriners Hospital is a world centre for the treatment of osteogenesis imperfecta (OI), caring for more than 250 patients with the rare genetic disorder. The multidisciplinary team includes a pediatrician, geneticist, orthopedic surgeon, physical and occupational therapists, a nurse and social worker. The clinic is also known for Dr. Francis Glorieux's pioneering use (starting in 1992) of bisphosphonates to increase bone density in children with OI. The goal of rodding is to correct deformed or fractured bone and protect against future fractures. Children typically undergo the surgery at 18 months to two years, when they first try to stand. Telescopic rods that elongate during growth offer longer lasting protection and have been used for decades. But the traditional system requires incisions at both ends of the femur to insert the parts of the rod, Dr. Fassier said. "What is the point of opening a knee joint in a patient who may develop knee joint problems in future? ?With the new rod, it's like any femoral rod?everything is done from the top. And osteotomies (to straighten deformed bone) whenever possible are done through the skin, through 2 mm incisions.? The less invasive approach also reduces blood loss and post-operative pain, he said. He and Dr. Duval, an orthopedic surgeon at Brtme-Missisquoi-Perkins Hospital in Cowansville, Que., started developing the new rod in the mid-1990s and began implanting it in March 2000. The steel rod consists of a solid "male" component with a screw at the distal end and a hollow "female" component with a screw at the proximal end. After reaming of the intramedullary canal and alignment of the bone, the male rod is driven distally and screwed into the distal epiphysis. The female rod is then slid over the male rod and locked proximally into the greater trochanter. The child is put in a posterior splint for three weeks instead of the usual six weeks of immobilization. After the cast is removed and replaced by a knee-ankle-foot orthosis, intensive physiotherapy can start. At the meeting, Dr. Fassier presented results at an average followup of 14.7 months in 21 patients who received 31 rods. At followup, 17 of the children were classified as household (nine), community (four) or therapeutic ambulators (four). There were no fractures, but this may also have been due to bisphosphonate therapy. The complication rate was 32% (10 of 31 rods) and the reoperation rate was 16% (five rods). Complications included protrusion of the male rod into the knee joint and migrating, nontelescoping or broken rods. Dr. Fassier said these figures compare favourably with those reported in the literature for telescopic rods?a 39% to 72% complication rate and a 10% to 40% reoperation rate?and at least some of the complications were related to the learning curve. Precise placement of the male rod in the distal epiphysis is crucial.
Filed under rodding, Τηλεσκοπικοί ενδομυελικοί ήλοι
New telescopic system for treatment of bone deformities
cleared by US-FDA and Canadian-TPDOctober 1st, 2004 - Montreal, Canada ? Pega Medical announces that it has been granted 510(k) clearance from the U.S. Food and Drug Administration (FDA) and an Amendment to its licence from the Canadian Therapeutic Product Directorate to market its new LON and SPS series of implants to complete its full line of the Fassier-Duval Telescopic IM Nail System. This novel device, used for the surgical treatment of bone deformities and fractures in patients suffering from Osteogenesis Imperfecta (OI), limb length discrepancy (LLD) and other bone deformities, now offers the surgeon a full range of options for the treatment of lower and upper extremeties.
New Indications
Besides OI the new implants completing the Fassier-Duval line will facilitate its use in Lengthening Over Nail, as well as treatment of Tibial Pseudoarthrosis. OI is a genetic disorder whereby the body of the affected patient either does not produce enough collagen or produces collagen of a poor quality, resulting in extreme bonfragility or what is known as brittle bones, i.e.: bones that fracture repeatedly and easily. For example, a child with severe OI could fracture a leg whilst turning in their sleep. Various treatments exist, including drugs, to aid the production of bone mass, and surgery to help straighten bones and prevent fractures. Bone lengthening and reconstruction procedures are commonly used in cases of Leg Length Differences; Arm Length Differences; Birth Defects (Congenital Deformities); Posttraumatic Bone Deformities; Non- Healing Fractures (Nonunions); Bone Loss From Tumor, Trauma, or Infection; Congenital Pseudarthrosis; Achondroplasia and Other Skeletal Dysplasias; etc. Improving the treatment of Pediatric patients worldwide - About the Fassier-Duval Telescopic IM Nail System. The Fassier-Duval Telescopic IM Nail System is an endomedular device aiding patients living with OI. Unlike other commercially available rods, the telescoping range of the F-D system has been increased as has the stability and fixation of the rod, reducing the necessity of revision surgery. The rehabilitation time post-op is reduced compared to that of other systems due to a minimally invasive technique and because the articular joints are unaffected by the surgery. Both reoperation and complication rates at 4 years has been reduced by 3- fold when compared to competitive devices. Initially developed by a bio-engineering company (Pega Medical Inc.) and Drs. Francois Fassier (Montreal Shriners Hospital) and Pierre Duval (BMP Hospital) as an alternative telescopic rodding system for surgical treatment of OI, the system has now extended its line of components by incorporating ideas and principles of Dr. Dror Paley (Rubin Institute, Baltimore) to improve the outcome for patients requiring bone lengthening procedures. The technique of lengthening over nails (LON) was developed in Maryland in 1990. The rationale behind this method is to reduce external fixation time. At the time of surgery, the intramedullary nail (metal rod) is inserted into the central hollow part of the bone. An external fixator is also applied to the bone. The lengthening is performed with the external fixator, and the F-D telescopic nail expands as distraction osteogenesis occurs. The external fixator is needed to perform the actual lengthening. Once the length is achieved, the external fixator can be removed in the operating room. The full consolidation of the distraction gap proceeds under the protection of the rod since it also prevents any bending, breaking after removal of the external fixator. Growth of the pediatric patient continues normally as the telescopic rod follows the bones natural growth. The external fixation treatment time is reduced by approximately one-half to two-thirds of what it would be if no nail were used. Using the nail also avoids the need for a cast or a brace after removal. A comparison between the LON method and the Ilizarov method showed that the recovery rate of knee motion after LON was 2.2 times faster than after the Ilizarov method. Over 300 implants have been used to date to treat patients across US, Canada, Spain, Belgium, Kuwait, Peru, Ecuador, and Slovenia.About Pega Medical
Pega Medical is an ISO 13485-certified privately held company based in Montreal specializing in the design, development, evaluation and manufacturing of orthopaedic medical devices. The company plans to launch the additional components into the world market in Q.1 of 2005. For further information: Ariel Dujovne, President, Pega Medical Inc. 9260 Viau blvd., Montreal, Quebec, CANADA Tel: (514) 322 8560 Fax (514) 328 9548 adujovne@pegamedical.com, www.pegamedical.comFiled under rodding, Τηλεσκοπικοί ενδομυελικοί ήλοι
Χειρουργική επέμβαση με τηλεσκοπικές ενδομυελικές ράβδους Fassier-Duval
Οι ενδομυελικές ράβδοι των Fassier και Duval (F-D rods) χρησιμοποιούνται πλέον στις περισσότερες χειρουργικές επεμβάσεις για παιδιά με ατελή οστεογένεση.Μια τηλεσκοπική ενδομυελική ράβδος που εφεύρε μια ομάδα Καναδών ορθοπεδικών χειρούργων υπόσχεται την ενίσχυση των μηρών των παιδιών με ατελή οστεογένεση (osteogenesis imperfecta), ενδεχομένως με λιγότερα περιπλοκές και επαναληπτικές χειρουργικές επεμβάσεις από ότι η παραδοσιακή τεχνική. Η συσκευή αναπτύχθηκε από τους Drs Franηois Fassier και Pierre Duval, μαζί με την Pegamedical, μια εταιρία του Μόντρεαλ που ειδικεύεται στις ορθοπεδικές συσκευές. Ο Dr Fassier είναι παιδο- ορθοπεδικός χειρούργος και προϊστάμενος του προσωπικού στο νοσοκομείο Shriners για παιδιά στο Μόντρεαλ. Είναι επίσης καθηγητής της χειρουργικής στο πανεπιστήμιο McGill. Το νοσοκομείο Shriners είναι ένα παγκόσμιο κέντρο για τη θεραπεία της ατελούς οστεογένεσης (osteogenesis imperfecta, OI), που φροντίζει για περισσότερους από 250 ασθενείς με τη σπάνια αυτή γενετική αναταραχή. Η πολλών ειδικοτήτων ομάδα περιλαμβάνει έναν παιδίατρο, έναν γενετιστή, έναν ορθοπεδικό χειρούργο, φυσικούς και εργοθεραπευτές, μια νοσοκόμα και έναν κοινωνικό λειτουργό. Η κλινική είναι επίσης γνωστή για την πρωτοποριακή χρήση των διφωσφωνικών (bisphosphonates) για την αύξηση της οστικής πυκνότητας στα παιδιά με OI από τον Dr. Francis Glorieux, ο οποίος έχει ξεκινήσει την εφαρμογή τέτοιας αγωγής σε παιδιά από το 1992. Ο στόχος της χειρουργικής επέμβασης rodding είναι να διορθώσει ένα παραμορφωμένο ή με κάταγμα οστό και να προστατέψει το οστό από μελλοντικά κατάγματα. Τα παιδιά μπορούν να υποβληθούν σε αυτήν την χειρουργική επέμβαση τυπικά από την ηλικία των 18 μηνών έως 2 ετών, όταν προσπαθούν να σταθούν για πρώτη φορά. Οι τηλεσκοπικές ράβδοι που μπορούν να επιμηκύνονται κατά τη διάρκεια της ανάπτυξης του παιδιού προσφέρουν μεγαλύτερης διάρκειας προστασία και χρησιμοποιούνται για δεκαετίες. Αλλά το παραδοσιακό σύστημα απαιτεί τομές και στις δύο άκρες του μηρού για να παρεμβληθούν τα μέρη της ενδομυελικής ράβδου. Ποιο είναι το νόημα του να ανοίξεις μια άρθρωση σε γόνατο σε έναν ασθενή που μπορεί να αναπτύξει συνήθη προβλήματα με τις αρθρώσεις των γονάτων του στο μέλλον; Με τη νέα ράβδο, είναι όπως με οποιαδήποτε άλλη μηριαία ενδομυελική ράβδο, όλα γίνονται από την κορυφή. Και τομές στο οστό (για να ισιώσουν το παραμορφωμένο οστό) , όποτε είναι δυνατόν, γίνεται μέσω του δέρματος, μέσω των τομών 2 χιλ. Αυτή η λιγότερο επεμβατική μέθοδος μειώνει επίσης την απώλεια αίματος και τον μετεγχειρητικό πόνο. Ο Dr Fassier και ο Dr. Duval, ένας ορθοπεδικός χειρούργος στο νοσοκομείο Brτme-Missisquoi-Perkins στο Cowansville, Que., άρχισαν την ανάπτυξη της νέας αυτής ράβδου στα μέσα της δεκαετίας του '90 και άρχισαν την χρησιμοποίησή της τον Μάρτιο του 2000. Η ράβδος χάλυβα αποτελείται από ένα συμπαγές «αρσενικό» μέρος με μια βίδα στο άκρο και ένα κοίλο «θηλυκό» μέρος με μια βίδα στο εγγύτατο τέλος. Μετά από τη διεύρυνση του ενδομυελικού καναλιού και της ευθυγράμμισης του οστού, η αρσενική ράβδος οδηγείται και βιδώνεται στην επίφυση. Η θηλυκή ράβδος έπειτα «γλυστράει» πέρα από την αρσενική ράβδο και κλειδώνεται. Το παιδί τίθεται σε έναν μετεγχειρητικό νάρθηκα για τρεις εβδομάδες αντί των συνηθισμένων έξι εβδομάδων της ακινητοποίησης. Αφότου αφαιρεθεί ο νάρθηκας και αντικατασταθεί με μια όρθωση γόνατου-αστράγαλου-ποδιών, η εντατική φυσιοθεραπεία μπορεί πλέον να αρχίσει. Σε συνέδριο, ο Dr. Fassier παρουσίασε τα αποτελέσματα από μια μέση παρακολούθηση 14.7 μηνών σε 21 ασθενείς που έλαβαν 31 ράβδους. Δεν υπήρξε κανένα κάταγμα, αλλά αυτό μπορεί επίσης να οφειλόταν στη θεραπεία με διφωσφωνικά (bisphosphonate). Το ποσοστό επιπλοκών ήταν 32% (10 από τις 31 ράβδους) και το ποσοστό επανεγχείρησης ήταν 16% (πέντε από τις ράβδους). Οι περιπλοκές περιλάμβαναν την προεξοχή της αρσενικής ράβδου στην ένωση γονάτων και μετακίνηση, μη ανάπτυξη ή σπάσιμο της ράβδου. Ο Dr. Fassier είπε ότι αυτοί οι αριθμοί συγκρίνονται ευνοϊκά με εκείνους που αναφέρονται στη βιβλιογραφία για τις τηλεσκοπικές ράβδους: ένα ποσοστό επιπλοκών από 39% έως 72% και ένα ποσοστό επανεγχείρησης 10% με 40%, και τουλάχιστον μερικές από τις επιπλοκές αφορούσαν την καμπύλη εκμάθησης. Η ακριβής τοποθέτηση της αρσενικής ράβδου στο ακραίο επίφυση είναι κρίσιμη.
- Oι ενδομυελικές ράβδοι των Fassier και Duval (FD-rods)
- Γιατί οι ενδομυελικές ράβδοι των Fassier και Duval είναι καλύτερες στην περίπτωση της ατελούς οστεογένεσης
- Από την σελίδα της Pedamedical:
- Χειρουργικές τεχνικές (PDF)
- Video παρουσίαση σε QuickTime Movie
- FAQ σε PDF για ασθενείς και για γιατρούς
 Κάντε κλικ εδώ για να γίνετε μέλος των OIparents
Κάντε κλικ εδώ για να γίνετε μέλος των OIparents{kind=link}
{kind=link}
{kind=link}